CBN (cannabinol) was the first cannabinoid to be chemically isolated, published in 1899, even before THC was identified. For decades it was interpreted as a sign of degradation: its presence in a sample indicated that the material had aged poorly. That approach changed when researchers began studying its own mechanism of action and understood that its effects are not an unwanted by-product but a differentiated profile.
Unlike THC or CBD, CBN is not a cannabinoid the plant produces actively. It forms through the degradation of THC upon exposure to oxygen, light and heat. That makes it a particular case within the cannabinoid family: its presence in a product depends neither on cultivation nor on genetics, but on how the material has been stored and processed.
Its effects profile is predominantly physical and sedative, with much lower psychoactivity than THC. Those characteristics have positioned it as the reference cannabinoid for insomnia management, but its interest extends well beyond that specific application.
In this article we explain what CBN is at a molecular level, what effects it produces and for which applications evidence exists, how it compares with THC and CBD in the context of sleep, and how to obtain and use it in a controlled way.
What is CBN?
CBN is not a cannabinoid that the cannabis plant synthesises actively. It is the product of THC degradation. When THC oxidises, it loses hydrogen from its molecular structure and converts into CBN. The process is spontaneous and irreversible.
In a freshly harvested plant, CBN is practically non-existent. The immediate precursor is THCA, the acidic form of THC present in the living plant. As it dries and cures, THCA converts into THC. From that point, if the material continues to be exposed to oxygen, ultraviolet light or heat, the THC begins to degrade into CBN.
The three agents that accelerate this conversion act in different ways. Oxygen is the main driver: oxidation is the central mechanism of the transformation. UV light breaks specific bonds in the THC molecule more rapidly than air exposure alone. Heat accelerates both processes, but is the hardest to control: at high temperatures, terpenes volatilise before the THC has had time to convert into CBN, yielding unevenly degraded material.
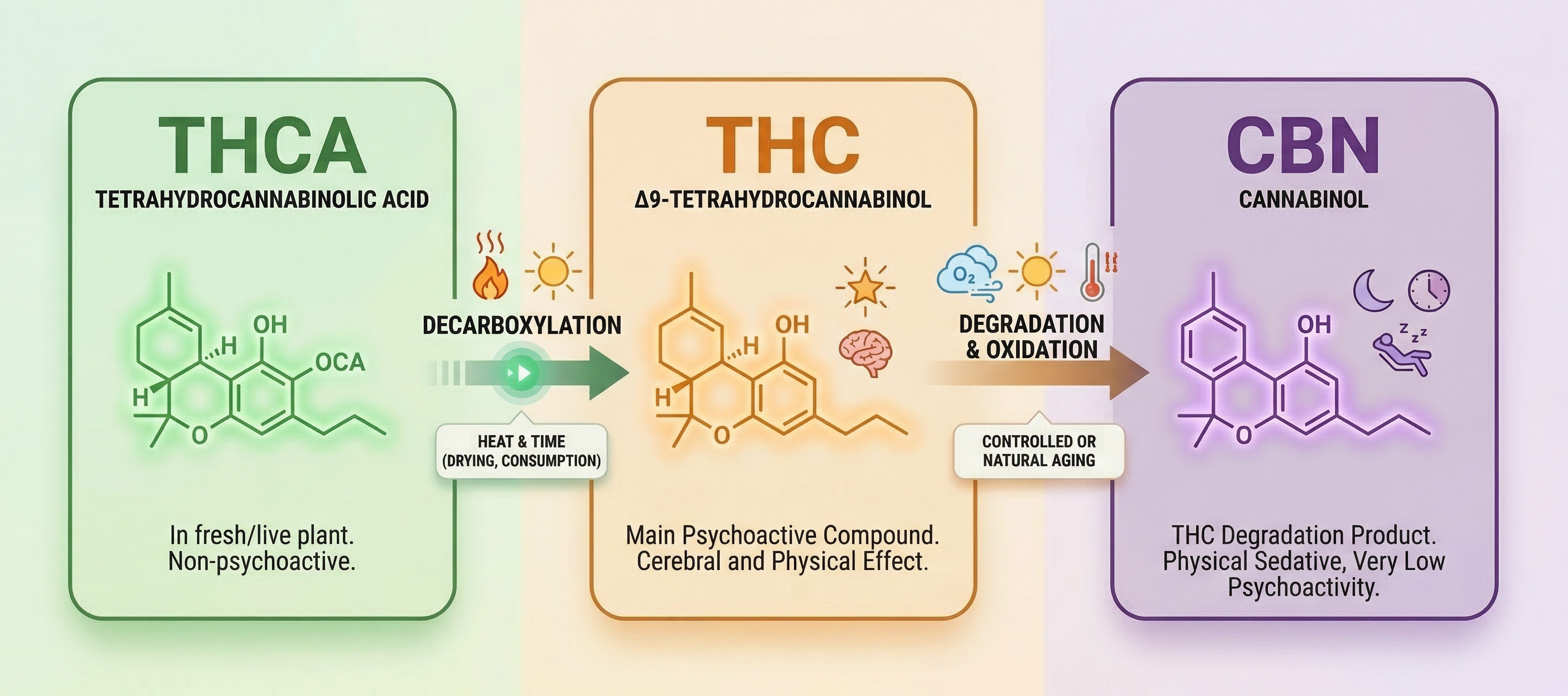
From THCA to CBN: the two transformations that occur after harvest and the agents that trigger them.
The difference between spontaneous degradation and controlled conversion lies precisely in this: during natural degradation, the material ages without control, the terpene profile is destroyed and the conversion of THC into CBN is partial and irregular. Controlled conversion aims to direct that process to maximise CBN while preserving as much of the remaining profile as possible.
In terms of its mechanism of action, CBN is a partial and weak agonist of CB1 receptors, the same ones THC acts upon. THC activates them strongly, producing the well-known psychoactive effects. CBN activates them far more mildly: its psychoactive potency is significantly lower than that of THC. This difference in CB1 affinity explains why its effects are predominantly physical and sedative rather than cerebral.
In a freshly harvested plant, CBN is practically non-existent. Its final concentration depends on processing, not on genetics or cultivation.
Effects of CBN
The effect most consistently associated with CBN in observational studies and user experience is physical sedation. It does not produce the mental relaxation characteristic of THC nor the anxiety reduction associated with CBD. Its action concentrates on the somatic nervous system: it relaxes the musculature, reduces physical activation and facilitates the onset of sleep without generating the altered mental state that accompanies THC. Controlled clinical trials in humans are still scarce, so the evidence on these effects remains preliminary.
That distinction is relevant for insomnia. THC can help bring on sleep, but in some people it activates thoughts, raises the pulse or generates anxiety — counterproductive effects when the goal is to switch off. CBN does not share that documented pattern. Its low affinity for CB1 means the psychoactive component is minimal and the predominant effect is physical quieting.
Another differential aspect frequently reported is the absence of cognitive hangover. Classic hypnotic drugs, and also high doses of THC, can leave a feeling of grogginess or mental sluggishness the following day. With CBN that effect is reported less frequently, probably because its half-life is shorter and its action on the central nervous system more limited, though this causal relationship has not been formally established. In practice, the doses needed to achieve the sedative effect do not reach the psychoactive threshold in the majority of users.
One final factor that conditions its efficacy is the presence of terpenes. CBN does not act in a vacuum: terpenes such as myrcene, present in many indica varieties, or linalool, also found in lavender, have their own sedative properties and act synergistically with CBN. A material that has lost its terpenes through poorly controlled degradation will produce less sedative effect even if it contains a significant amount of CBN.
CBN's psychoactive potency is estimated at around 10% of that of THC. In practice, that means the doses needed to achieve sedation do not reach the psychoactive threshold in the majority of users.
Applications of cannabinol beyond insomnia
CBN is primarily associated with insomnia management, but research points to a broader effects profile. Most available studies are in vitro or in animal models, meaning the results are indicative and cannot be directly translated into clinical conclusions in humans. Nevertheless, some lines of research show enough consistency to be described honestly.
Antibacterial properties
This is probably the area with the most solid evidence outside of sleep. A study published in 2008 by researchers at the University of Westminster evaluated five major cannabinoids against methicillin-resistant Staphylococcus aureus (MRSA) strains, a bacterium that poses a serious clinical problem due to its resistance to conventional antibiotics. CBN was one of the cannabinoids that showed relevant inhibitory activity in that in vitro context.
The exact mechanism is not fully understood, but the results positioned cannabinoids, including CBN, as candidates to explore in the development of new antibacterial agents. The distance between an in vitro result and a clinical treatment is considerable, but the finding is concrete enough to be taken seriously.
Anti-inflammatory and analgesic effect
CBN interacts with the endocannabinoid system, which has a well-established role in the regulation of the inflammatory response. Studies in animal models have observed a reduction in inflammatory markers following CBN administration. Activity on TRPV1 and TRPV2 receptors, involved in pain perception and local inflammatory response, has also been documented.
The analgesic effect of CBN has not been studied as extensively as that of CBD, but there are indications that it acts through complementary pathways, opening the possibility of synergistic effects in combination with other cannabinoids.
Appetite stimulation
This effect may come as a surprise if CBN is associated exclusively with sedation, but studies in rats document an increase in appetite following CBN administration, even in the absence of THC. This is a relevant finding because CBD has the opposite effect: it tends to reduce appetite in some contexts. CBN could be of interest in situations where loss of appetite is a problem, though this effect has not yet been well characterised in humans.
CBN and THC are not mutually exclusive profiles
THC and CBN are not mutually exclusive options: they are the same material at two different points in its cycle. A grower who already has flower with a high THC concentration also has the raw material to produce CBN. The question is not which to choose but when and for what purpose to use each part of the harvest.
Unconverted THC is effective at inducing sleep, but reduces the REM phase with continued use and in some people generates anxiety or a racing heart just before bed. CBN obtained through controlled conversion acts differently: predominantly physical sedation, without the psychoactive component and without documented interference with REM sleep, though human studies are still insufficient to rule that out with certainty.
These are not equivalent or interchangeable profiles. CBN does not accelerate sleep onset as rapidly as THC, but it also does not carry its documented limitations. A balanced ratio of both — for example 1:1 as an indicative starting point — can combine THC's ability to accelerate sleep onset with CBN's physical sedative effect: THC provides speed of onset and CBN stabilises the effect and moderates the psychoactive component. Added to this is the role of the sedative terpenes that survive the process: myrcene and linalool act synergistically with CBN and make the difference between a functional material and one that has simply aged.
Recent studies, including those from Radicle Science published in 2023, suggest that isolated CBN may have a more limited sedative effect than previously assumed. CBN's hypnotic action appears to depend largely on its interaction with other compounds in the spectrum: residual THC, sedative terpenes, or both. In other words, the entourage effect is not an optional add-on to CBN but probably the necessary condition for its hypnotic action to be meaningful. This reinforces the logic of controlled conversion over an isolate: what is sought is not to accumulate CBN at any cost but to preserve the complete profile that makes that CBN work.
How to convert THC into CBN
The starting material
The process works with flower, trim or any plant material that has started from a sufficient THC concentration. The higher the initial THC content, the greater the conversion potential to CBN. A material with 15–20% THC to start with will produce more CBN than one with 5%. The starting genetics sets the ceiling for conversion: high-THC varieties such as CandyGaz or Brain Cake offer more margin to obtain CBN in quantity.
Trim, though it has lower concentration per gram than flower, is a common starting material precisely because it tends to be abundant and dedicating it to this process does not mean sacrificing higher-value material.
What does not work is starting from material that has already been extracted or from which the resin has been removed. The conversion requires the cannabinoids present in the plant material, not an empty substrate.
Do not use mouldy material
Degraded cannabis and substandard cannabis are not the same thing. Material that has aged under dry, uncontaminated conditions is suitable for conversion. Material with mould is not.
The common mistake is assuming that the oven's heat eliminates any risk. It does not. Mycotoxins produced by mould are thermostable: they survive the temperatures of the baking protocol and remain toxic in the resulting material. Mould is visually detectable in most cases, through the presence of white, grey or greenish spots and a damp or earthy smell that does not match the terpene profile of cannabis. If in doubt, the material is not used.
Directed oxidation
The process differs from standard decarboxylation: whereas 10–15 minutes suffice to activate THC, conversion to CBN requires more prolonged exposure for oxidation to advance significantly.
The transformation of THC into CBN is an oxidation reaction. THC loses hydrogen by reacting with the surrounding oxygen. Heat does not produce CBN on its own: what it does is accelerate that reaction. Without available oxygen, heat simply degrades the material without generating CBN in any significant quantity. That is why the process requires exposure to air, not a sealed environment.
Temperature and terpenes
Terpenes do not all evaporate at the same temperature. The most volatile monoterpenes, responsible for fresh and citrusy aromas, begin to be lost from 70°C onwards. But the terpenes most relevant to the sedative profile have much higher boiling points: myrcene is around 167°C and linalool around 198°C. At 120°C, terpenes are lost, but not the ones that matter for insomnia.
CBN forms efficiently from 100–120°C upwards. Below that range, conversion is very slow and incomplete. Above 140°C, sedative terpenes start to be compromised and the yield curve reverses: the CBN being formed begins to degrade into inactive compounds faster than new CBN is generated.
There is an alternative for those who prioritise preserving the full terpene profile: working at 90–100°C for a longer period, between three and four hours. The conversion of THC into CBN is less efficient, but the loss of volatile terpenes is lower. It is a trade-off between conversion speed and profile preservation.
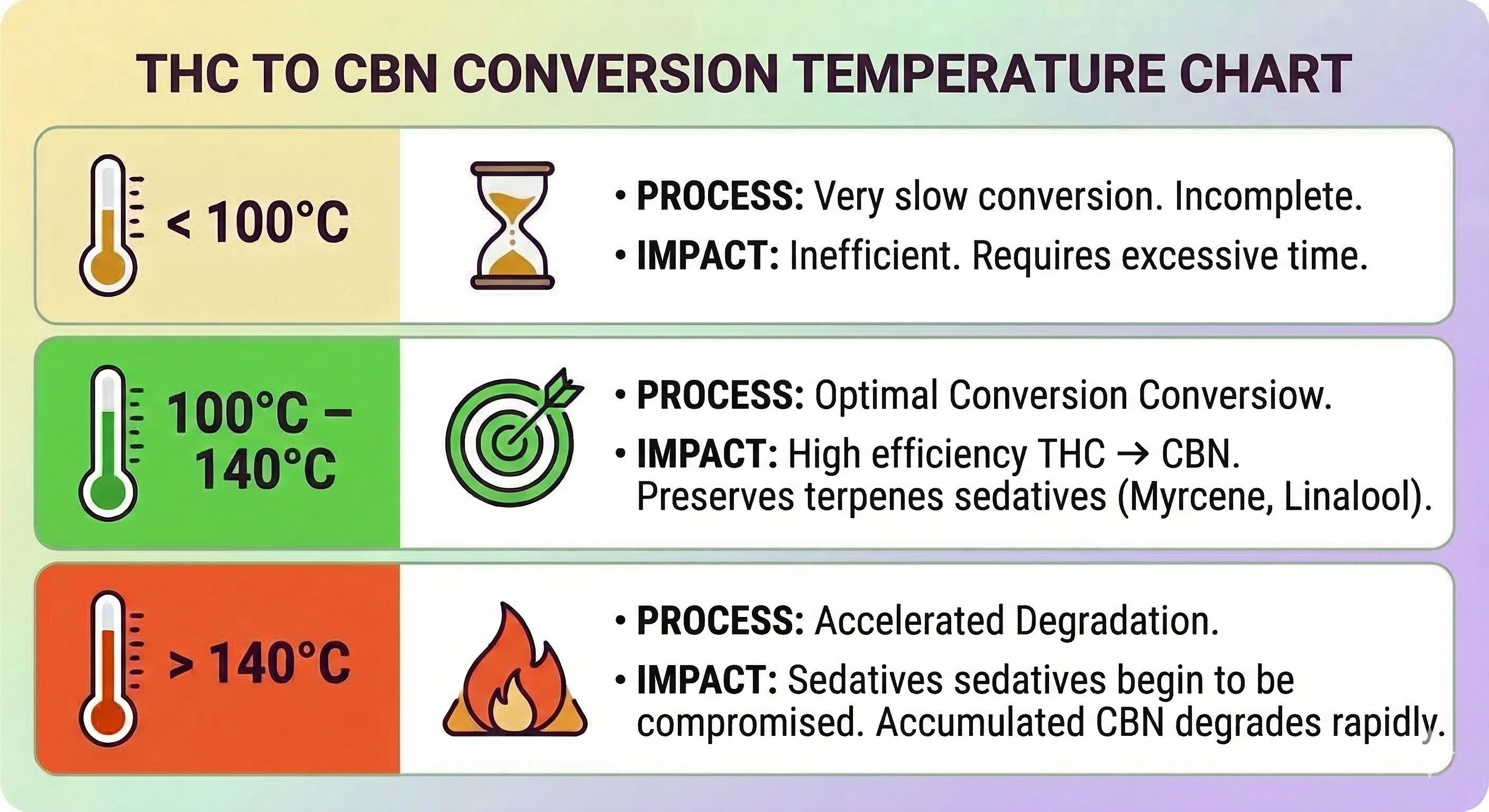
The three temperature ranges and their effect on THC-to-CBN conversion and the preservation of sedative terpenes.
Baking protocol
The most reproducible method in a home setting is baking in a conventional oven. Before starting, the material must be thoroughly dry: residual moisture generates steam that interferes with heat transfer and produces uneven conversion. If the material has been cured recently, it is worth leaving it to dry at room temperature for a day or two. The process conditions are:
- Temperature: 120°C
- Time: 60 to 90 minutes
- Material spread evenly on the tray, without piling up
- Oven without forced fan: forced air creates uneven temperature spots and oxidises the material irregularly
The choice of 120°C is not arbitrary: it is the point at which conversion of THC into CBN is efficient and the sedative terpenes — myrcene and linalool — remain below their volatilisation threshold.
The most reliable visual indicator is the colour change: the material shifts from a dull green to a progressive tobacco brown. A uniform dark brown indicates the process is at its limit. Black or very dark patches in parts indicate excess temperature or time.
It is worth noting that domestic ovens show real variability in heat distribution. Ambient humidity and the thickness of the material can also affect the outcome.
At 120°C, THC-to-CBN conversion is efficient and sedative terpenes are preserved. Above 140°C the process reverses: CBN degrades faster than it forms.
Cannabinol has a conversion ceiling
The transformation of THC into CBN is not indefinite. Beyond a certain point, CBN continues to degrade into inactive compounds that have no sedative effect or any other meaningful effect. That ceiling is reached through excess temperature, excess time, or both.
Above 140°C or after more than three hours of heat exposure, the conversion curve begins to reverse: the accumulated CBN degrades faster than new CBN forms. The resulting material may appear dark and have a burnt smell, and its efficacy will be significantly lower than that of material converted within the correct parameters.
The protocol does not improve the longer it is applied. The optimal window exists and has an upper limit just as relevant as the lower one.
Verifying the result
The colour change during baking is the available visual indicator, but it has limitations: two materials showing the same colour can have different CBN concentrations depending on genetics, initial moisture content and the uniformity of the heat applied. The colour confirms that a transformation has occurred, not its magnitude.
For those who want more certainty, thin-layer chromatography (TLC) test kits are available from laboratory supply shops or some specialist cannabis retailers. They do not give an exact concentration, but allow confirmation of CBN's presence and an estimate of whether conversion has been significant by comparing the intensity of the THC and CBN spots on the plate. It is an indicative method, not an analytical one, but it is the only one accessible outside a laboratory.
Post-conversion storage
Once conversion is complete, degradation does not stop. CBN continues to oxidise if the material is left exposed to air, light or heat. UV light in particular accelerates oxidation at room temperature, which is why transparent containers are not suitable for storage even if the material is kept cool.
Optimal conditions are: opaque airtight container, stable and low temperature, no humidity. Under those conditions the profile remains stable for several weeks. Any exposure to air or light after conversion compromises the material's efficacy in the short term.
From converted material to oral format
The baking protocol produces decarboxylated material with a high proportion of CBN. That material is not taken directly: the oral route requires cannabinoids to be dissolved in a fat, as they are lipophilic molecules that the digestive system does not absorb efficiently in the absence of lipids.
Fat extraction
 Sherpa SEO, CC BY 3.0, via Wikimedia Commons
Sherpa SEO, CC BY 3.0, via Wikimedia Commons
{kind=link}
The most straightforward method for home use is oil infusion. Extra virgin olive oil and coconut oil are the most widely used due to their saturated and unsaturated fatty acid profile, which dissolves cannabinoids well. Coconut oil has the advantage of being solid at room temperature, which makes dosing easier when working with a scale.
The infusion conditions are:
- Ratio: 5 grams of material per 100 ml of oil as a starting point. With high-potency starting material this can be reduced to 3 grams; with low-potency material or trim, increase to up to 7 grams.
- Temperature: between 70 and 80°C
- Time: 60 to 90 minutes
A higher ratio does not improve results linearly: the oil has a practical saturation limit and excess material does not contribute additional cannabinoids. Above 90°C the oil begins to oxidise and any remaining terpenes volatilise.
The most controllable method at home is a double boiler: the oil and material are placed in a sealed container set inside water kept at a constant temperature. This avoids the temperature spikes that occur with direct contact with a heat source.
After infusion, the plant material is filtered through a fine strainer or cheesecloth. The leftover material is discarded: it has given up its cannabinoids to the oil and has no further use.
Dosing the resulting oil
Oil produced at home does not have a precisely known CBN concentration. There is no way to determine how much CBN each millilitre contains without chromatographic analysis. That requires working with a titration logic: start with a low dose, observe the effect and adjust progressively.
A reasonable starting point is 1–2 ml of oil. From there, adjust in increments of 0.5 ml according to the response. The goal is not to find the maximum tolerable dose but the minimum effective one, which varies according to metabolism, body weight and the concentration of the oil.
How to take CBN
The cannabinol action window
CBN is most commonly consumed orally. In commercial products it appears in oil with a declared concentration, in capsules or incorporated into edibles. Oil made through controlled conversion at home follows the same route, with the difference that the concentration is unknown and dosing requires progressive adjustment.
Unlike inhalation, whose effect is almost immediate, the oral route requires the digestive system to process the material before cannabinoids pass into the bloodstream.
The time to peak effect ranges between 45 and 90 minutes depending on individual metabolism and stomach contents. Taking it right at bedtime means the effect will arrive after an hour spent lying in bed unable to sleep, producing the opposite of the intended result. The peak effect arrives before sleep is the objective if taken 45 to 60 minutes before going to bed.
THC reduces the REM phase with continued use. That effect has not been documented with CBN, though human research is still insufficient to rule it out with certainty.
The starting dose
Although CBN has very low psychoactivity, its physical sedative effect is considerable. An excess does not produce a high, but can generate a feeling of heaviness or lethargy that extends into the following morning if the body is not accustomed to it.
For commercial products with a concentration declared on the label, the usual starting point is between 5 and 10 mg. For oil made at home, where the concentration is unknown, the starting point is volume: 1–2 ml, adjusting in increments of 0.5 ml according to the response. In both cases the principle is the same: start low and adjust, because bioavailability varies according to format, metabolism and stomach contents.
Alcohol and fats in absorption and sleep
Alcohol and fats affect CBN in different ways, but both condition the final outcome.
Alcohol potentiates CBN's sedative effect in an unpredictable way because it acts on the same central nervous system receptors. It also fragments sleep architecture in a specific way: it suppresses REM sleep in the first half of the night and generates a rebound in the second half, producing shallow and fragmented sleep even if the initial onset was quick. Combined with CBN, the result can be an intense initial sedation followed by poor-quality sleep.
Fats act on absorption, not on the effect itself. Cannabinoids are lipophilic molecules that are absorbed alongside the micelles formed during fat digestion. A very fat-heavy meal does not prevent absorption but slows and concentrates it, shifting the peak effect towards the middle of the night. The opposite case is equally relevant: taking it on an empty stomach significantly reduces absorption. A light meal with some fat offers the most predictable balance between absorption speed and completeness.
Screens after taking CBN
CBN facilitates physical relaxation but does not switch off mental activation. If, after taking it, one continues with intense screen exposure, a dissociation occurs between the physical and mental state: the body begins to give way but the brain remains active, which in some users generates an uncomfortable feeling of dizziness or disorientation. Reducing visual stimulation after taking CBN improves the transition to sleep.
Pharmacological interactions with CBN
The most direct interaction is with other central nervous system depressants: benzodiazepines, sedating antihistamines such as diphenhydramine, opioids and alcohol. The sedative effect compounds in an unpredictable way and can produce deeper sedation than intended. Anyone taking any of these drugs regularly should bear this in mind before using CBN.
Like other cannabinoids, CBN is metabolised via the hepatic CYP3A4 pathway and possibly CYP2C9. This creates a potential interaction with drugs that use the same pathways, including certain anticoagulants, statins and antidepressants. This interaction has not been specifically studied for CBN but is extrapolated from the general cannabinoid profile. Anyone taking drugs with hepatic metabolism should consult a doctor before using CBN.
CBN: a cannabinoid with a defined profile and a demanding process
CBN is a cannabinoid with a concrete effects profile and a mechanism of action differentiated from both THC and CBD. Its usefulness for insomnia is supported by observational studies and preliminary evidence, though controlled clinical research in humans remains scarce. What is clear is its mechanism: low CB1 affinity, predominantly physical sedation and the absence of the psychoactive component that makes THC less predictable for some people in the context of sleep.
Its distinctive quality relative to other cannabinoids is that it does not depend on cultivation or genetics: it depends on processing. That makes it accessible in ways that other minor cannabinoids are not, but it also demands a level of process control that makes the difference between a useful material and one that has simply degraded.
The most effective profile is not isolated CBN but CBN within a spectrum that preserves sedative terpenes and, depending on the case, a proportion of THC or CBD. Controlled conversion only makes sense when carried out with the goal of maximising that complete profile, not merely of accumulating CBN at any cost.
This article is for informational purposes only and does not constitute medical advice.
Sources
- Wood, Spivey and Easterfield. Isolation of cannabinol. Journal of the Chemical Society, 1899.
- Appendino et al. Antibacterial activity of cannabinoids against MRSA. Journal of Natural Products, 2008.
- Weydt et al. CBN and symptom progression in an ALS model. Amyotrophic Lateral Sclerosis, 2005.
- Pertwee. Pharmacology of cannabinoids at CB1 and CB2 receptors. British Journal of Pharmacology, 2008.
- Farrimond, Whalley and Williams. Effects of CBN and CBD on appetite in rats. Psychopharmacology, 2012.
- Mahadevan et al. Novel cannabinol probes for CB1 and CB2 cannabinoid receptors. Journal of Medicinal Chemistry, 2000.
- Radicle Science. Cannabinol (CBN) and sleep: a randomized, double-blind, placebo-controlled study. 2023.